find your solution.
search for solutions by category, industries, insights, and people.
search for solutions by category, industries, insights, and people.
search for solutions by category, industries, insights, and people.


The Centers for Medicare & Medicaid Services (CMS) Rural Health Transformation (RHT) Program represents the largest federal investment ever directed toward rural healthcare delivery. Authorized by the One Big Beautiful Bill Act, the program commits $50 billion over five years (FY 2026–2030) to help states stabilize and modernize rural health systems, expand access to care, and strengthen workforce capacity. To manage this multi-year effort, CMS established the Office of Rural Health Transformation, which monitors state transformation plans and supports the effective use of program funds.
The scale of the investment reflects the urgency of the challenge. According to an annual study by Chartis, more than 40% of rural hospitals are operating at a loss, with 417 facilities considered “vulnerable to closure.” Against this backdrop, the RHT Program presents a rare opportunity to address longstanding structural challenges. It also introduces new operational, financial, and enterprise-level risks and heightened accountability tied to the scale, duration, and oversight of the program.
Organizations that pair strategic investment with disciplined governance and internal control practices will be best positioned to convert grant dollars into lasting operational improvements and measurable community health outcomes.
The RHT Program distributes $10 billion annually to all 50 states through cooperative agreements administered by CMS. Half of the funding is allocated equally among approved states, while the remaining 50% is distributed based on factors such as rural population, the concentration of rural health facilities, and hospital-specific conditions within each state.
First-year awards range from approximately $147 million to $281 million per state, reflecting differences in rural health needs and the scope of proposed transformation initiatives.
Across states, funded initiatives commonly focus on:
Collectively, these investments are designed to transform rural healthcare delivery ecosystems rather than provide short-term financial relief.
For rural hospitals and healthcare providers, the RHT Program opens access to capital at a scale rarely available through traditional grant programs. States can tailor funding strategies to local needs, enabling providers to pursue shared services, regional partnerships, and coordinated care models that strengthen long-term viability.
Workforce development stands at the center of many state plans. Grant recipients can invest in recruitment and retention strategies, training programs, and expanded use of community health workers, pharmacists, and other licensed professionals.
Equally important, RHT funding supports modernization efforts, ranging from facility upgrades to advanced technology platforms, which allow rural providers to deliver higher quality care closer to home.
While the opportunity is significant, participation in the RHT program materially changes the risk environment for rural healthcare organizations.
The RHT program is administered as a federal cooperative agreement, requiring intensive oversight, annual reapplications, updated budgets, and ongoing reporting between states and CMS. Many states (e.g., New York) explicitly warn that this model demands substantial administrative effort from sub‑awardees.
For healthcare systems with limited administrative capacity, additional staffing for reporting, documentation, and compliance monitoring can increase overhead and divert resources from clinical operations with a CMS-mandated 10% cap on administrative activities.
RHT funding has strict limitations on how funds may be used. Funds may not be used to supplant existing clinical funding, support construction or major building projects, cover pre-award costs, or satisfy other federal matching requirements. As a result, providers must track costs carefully to avoid federal disallowances that could require repayment.
Projects that fall outside allowable categories may still be strategically important but must be funded by working capital or other means, increasing financial exposure and the potential for clawbacks if documentation fails to demonstrate full compliance.
RHT funding ends after FY2030, creating only a five‑year window for transformation. Services, technology platforms, and workforce initiatives launched with grant support must be financially sustainable once funding ends.
Without careful planning, hospitals may face post grant instability, particularly if new programs rely solely on RHT funding, lack ongoing revenue streams, or operate within already thin margins that limit the ability to absorb continued costs.
Many rural providers enter the program with pre-existing financial strain, including high costs, limited market power, small economies of scale, constrained liquidity, and structural balance sheet weaknesses.
Grant participation requires upfront investment or co-investment, while reimbursement timing can create cash flow pressure. For organizations already operating with thin margins, these dynamics can unintentionally compound financial stress rather than alleviate it.
Taken together, these risks can reflect a fundamental shift in operating reality for rural healthcare organizations, as the scale, duration, and oversight of RHT funding elevate risk and require intentional governance and disciplined internal controls throughout the grant lifecycle.
Large federal grants bring expanded compliance, financial, and operational obligations. As stewards of public funds, recipients must maintain structured oversight and accountability aligned with CMS expectations. For rural hospitals and healthcare providers receiving RHT-related funding, this requires disciplined financial management and monthly, state-level compliance reporting on individual grants, covering expenditures, progress against approved plans, and required certifications.
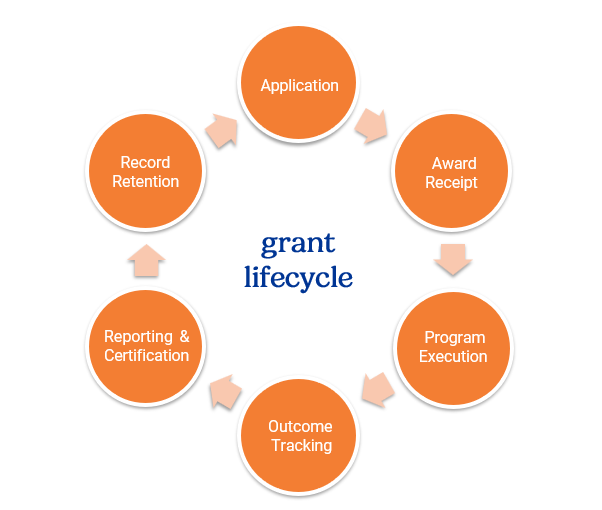
Strong internal controls are not only a federal requirement, but a foundational risk management necessity, safeguarding public funds and helping to protect providers from operational, financial, and reputational harm. A well-designed grant internal control framework provides end-to-end oversight across the grant lifecycle, promoting transparency, strengthening risk management, and supporting program performance from application through closeout as compliance demands intensify.
An effective framework focuses on:
Risk begins at application and continues through closeout. Effective internal controls provide continuous oversight across the grant lifecycle, creating a structured environment where operational, financial, and compliance risks are identified, monitored, and mitigated.
Risk begins at application and continues through closeout. Effective internal controls provide continuous oversight across the grant lifecycle, creating a structured environment where operational, financial, and compliance risks are identified, monitored, and mitigated.
Hospitals and healthcare providers that extract lasting value from RHT funding will approach it as a multi year transformation initiative, not a one time infusion of capital. Practical strategies include:
Strong controls help providers connect grant spending to long term operational resilience and community health outcomes.
The Elliott Davis Healthcare team supports rural hospitals and healthcare providers across the full grant lifecycle, from strategic planning and application support through compliance, governance, internal controls, and post-grant closeout validation. Our integrated approach helps organizations strengthen accountability while maximizing the long-term value of transformative federal funding.
Contact us today to start the conversation and learn more about the tools and processes we’ve built to support this initiative.
The information provided in this communication is of a general nature and should not be considered professional advice. You should not act upon the information provided without obtaining specific professional advice. The information above is subject to change.



.avif)

